Hallux Valgus (Bunions)


About the condition
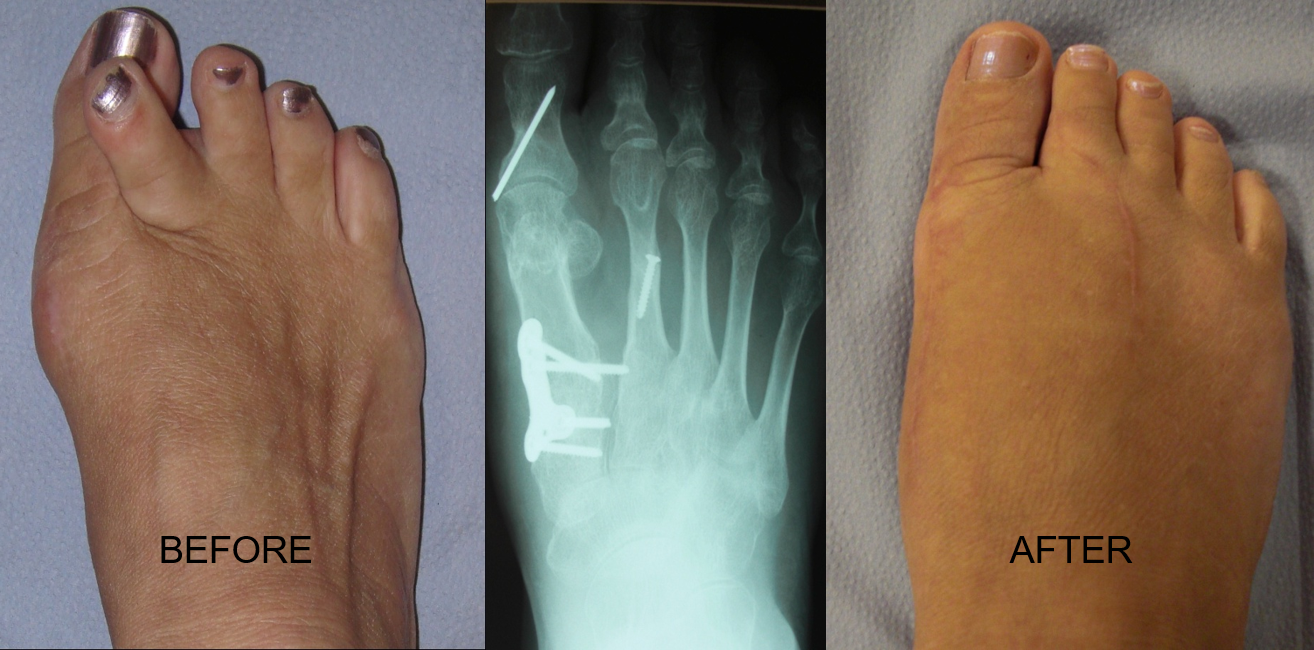
Hallux valgus — commonly called a bunion — is a progressive deformity of the big toe joint in which the great toe drifts laterally and a bony prominence forms on the inside of the forefoot. It is one of the most prevalent structural foot problems in adults, affecting an estimated 20–35% of the population and considerably more women than men.
The cause is usually multifactorial: hereditary joint shape, ligamentous laxity, biomechanical overload and, over years, footwear that crowds the forefoot. It is not caused solely by shoes, but tight or narrow footwear will accelerate progression once the deformity has begun.
Not every bunion needs surgery. Many patients are managed successfully for years with footwear modification, orthoses and activity advice. Surgery is considered when pain, function or footwear tolerance are meaningfully affected.
What patients notice
- •A visible bony bump on the inside of the forefoot at the big toe joint
- •Aching or burning pain over the joint, especially in enclosed shoes
- •Redness, swelling or inflamed bursa over the prominence
- •The great toe drifting towards or under the second toe
- •Callus or corn formation on the ball of the foot from altered loading
- •Difficulty finding comfortable footwear
Why timely assessment matters
- •Progressive worsening of the deformity and joint alignment over time
- •Secondary problems in the lesser toes, including hammer toes and crossover toe
- •Development of osteoarthritis in the first metatarsophalangeal joint
- •Transfer metatarsalgia — pain under the ball of the foot as load shifts
- •Chronic bursitis, skin breakdown or ulceration over the prominence
- •Reduced walking tolerance and activity levels
How we treat it
Footwear and activity advice
The starting point for most patients: shoes with a wide, deep toe box, a low heel and adequate cushioning. Simple changes can significantly reduce pain even when the deformity itself persists.
Orthoses and padding
Custom or prefabricated orthoses can offload the first ray, improve overall alignment and reduce secondary symptoms in the forefoot and heel.
Physiotherapy and mobilisation
Targeted stretching and strengthening — particularly of the intrinsic foot muscles and the first ray — can help maintain joint mobility and delay progression.
Minimally invasive bunion surgery
Percutaneous techniques allow the deformity to be corrected through very small incisions, with internal screw fixation and rapid mobilisation. Suitable for many mild to moderate deformities.
Open reconstructive surgery
For larger or more complex deformities, an open procedure allows precise realignment of the bones, joint capsule and soft tissues, with reliable long-term correction.
Joint-preserving vs joint-fusing procedures
Where arthritis is established, fusion of the first metatarsophalangeal joint may give the most durable pain relief. In earlier disease, joint-preserving osteotomies are usually preferred.
And why
Narrow, pointed or high-heeled shoes
Why: They compress the forefoot and push the great toe further out of alignment, accelerating deformity and inflaming the bursa.
Ignoring pain in the second toe
Why: Pain under or over the second toe often signals the bunion is destabilising the neighbouring joints — earlier assessment prevents cascade deformity.
Over-the-counter 'bunion correctors' as a cure
Why: Splints and toe spacers can be comfortable but do not reverse a structural deformity. Relying on them may delay effective treatment.
Aggressive self-treatment of overlying skin
Why: Cutting or filing callus and corns at home risks infection, particularly if circulation or sensation is impaired.
This page provides general information about the condition and is not a substitute for personalised clinical advice. Diagnosis and treatment planning should always follow an in-person consultation.
Discuss hallux valgus (bunions) with a consultant.
Book a consultation at Spire Parkway or an online review with Mr Stuart Metcalfe.